Online

Currently 54 countries are off-track to achieving the SDG target for under-five mortality, and more will fall behind if we do not act with urgency. Against this grim reality, other countries have made tremendous progress in cutting back preventable under-five mortality showing that with determination and strong technical and political leadership, progress is possible. The Child Health Task Force is excited to announce its first virtual conference to unite child health partners around how we address health inequities to enable children across the globe and throughout the life course to survive and thrive.
Thank you to all who joined us! Child health partners from around the world convened for a conversation on how we might address health inequities to enable children to survive and thrive. Inspiring speakers and expert practitioners, included:
- Keynote speaker Dr. Atul Gawande, Assistant Administrator for Global Health, USAID
- Professor Lisine Tuyisenge, Rwanda Paediatric Association
- Professor Hadiza Galadanci, Africa Center of Excellence for Population Health and Policy, Bayero University Kano, Nigeria
- Dr Queen Dube, Ministry of Health Malawi
- Dr. Sangeeta Yadav, Maulana Azad Medical College, New Delhi
- Dr. Anshu Banerjee, WHO
- Dr. Lu Wei Pearson, UNICEF
Agenda At-A-Glance
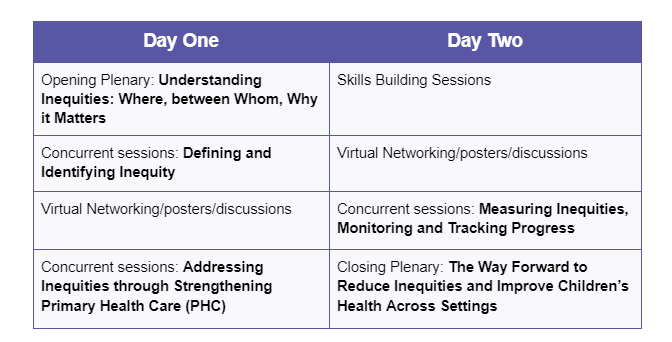
The plenary, concurrent sessions, and virtual conference site will be available in French and English.
Conference Objectives
- Identify key vulnerabilities and risk factors that perpetuate inequities in child health across the countries represented in the Task Force membership.
- Exchange promising and innovative programmatic and systems-strengthening solutions for reaching hard-to-reach children with lifesaving interventions.
- Share experiences, models, and frameworks for accountability, measuring, and evaluating progress in achieving child health equity.
- Gather inputs to develop recommendations for advocating for governments, global partners, and donors to commit to addressing inequities in child health through renewed energy and focus on child survival and wellbeing.
Thematic Tracks
Across the tracks, presentations will showcase research results, emerging evidence, tools, program approaches, partnerships, policy action, financing, successes, and implementation failures that will foster deep reflection, provoke dialogue and spur action to reach the unreached children.
1. Defining and identifying inequity
Children born in sub-Saharan Africa are 12 times more likely to die before their fifth birthday than children in high-income countries, a statistic that has barely changed over the past 30 years. We know these inequities exist, but in order to address them, we need to define, understand and identify children who are affected, including those in humanitarian contexts, crisis and fragile settings, urban slums, rural areas, caste, and ethnic or religious minorities, etc.
2. Addressing inequities through strengthening Primary Health Care (PHC)
Despite intractable implementation challenges and limited funding, some countries have made tremendous progress in improving health outcomes. These countries have strengthened the critical elements of the PHC systems as an inclusive health system.
3. Measuring inequities, monitoring and tracking progress
A major challenge has been establishing sustainable, quality mechanisms for measuring inequities and tracking progress.
Conference Materials
No child should die of a preventable and treatable illness. While progress has stalled in many countries, a few countries have made tremendous progress in reducing preventable under-five mortality. These countries are beacons of hope. However, even in places where progress is noticeable, some children are left behind as health systems fail to meet their needs. During the next two days, participants will enhance their understanding of inequity in child health and how to define, address, and track progress as we also reaffirm our commitment to ending preventable child deaths for all children.
Presenters
- Dr. Atul Gawande, Assistant Administrator for Global Health, USAID
- Dr. Dyness Kasungami, Project Director, Child Health Task Force
- Prof. Lisine Tuyisenge, President and Legal Representative, Rwanda Pediatric Association
- Professor Hadiza Galadanci, Professor of Obstetrics and Gynaecology, Department of Obstetrics and Gynaecology, Aminu Kano Teaching Hospital, Director, Africa Center of Excellence for Population Health and Policy, Bayero University Kano, Nigeria
- Dr Anshu Banerjee, Director, Maternal, Newborn, Child and Adolescent Health and Aging
Moderator
- Mercy Juma, BBC News East Africa Correspondent
There are at least 240 million children with disabilities globally, and they are 3x as likely to be malnourished compared to children without disabilities. Children with disabilities are often excluded from programs and services. Their families and caregivers may need new skills to nourish them, and face higher rates of poverty, stress, and food insecurity. Children with disabilities are more likely to be in residential care, which increases their risk of malnutrition.
A lack of data on disability and nutrition makes it difficult for policy makers, health systems, and the nutrition sector from developing solutions to fulfill their rights. This presentation will:
1. Describe inequities faced by children with disabilities in nutrition and feeding, including root causes, impact, and systems issues
2. Share experiences from three multi-sectoral programs: linking developmental and nutrition screening in Lesotho; strengthening family care and nutrition in Uganda; and supporting nutrition and feeding for children with disabilities and families in Zambia.
3. Offer recommendations for policy, services, and investments We will use literature, key informant interviews, and data from Count Me In, SPOON’s app that guides trained users through growth monitoring, feeding assessment, and anemia screening.
Count Me In produces site- and country-level data, disaggregated by disability. Our data show that children with disabilities are at high risk of feeding difficulties, unsafe feeding practices, and malnutrition, including stunting, wasting, underweight, and anemia.
The audience will leave this presentation with a clearer understanding of the inequities in nutrition and feeding for children with disabilities and ideas for how they can change their work to include children with disabilities.
Presenters
- Dr. Zeina Makhoul, Nutrition Scientist, SPOON
- Ms. Pamela Magero, Master Trainer, SPOON
- Watson Mwandileya, Child Protection and Health Program Officer, Access to Health Zambia
- Nkhasi Sefuthi, LLM, Executive Director, Lesotho National Federation of Organisations of the Disabled
Moderator
- Carolyn Moore, Policy and Advocacy Advisor, SPOON
In 2021, 25 million children did not receive one or more doses of the vaccine against diphtheria-tetanus and pertussis (DTP) and 18 million of those did not receive even the first dose of DTP-containing vaccine, leaving millions of children vulnerable to preventable under-five mortality. These children and their families face multiple vulnerabilities and risk factors that result in inequitable access to and utilization of primary health care services, including immunization. SDG targets cannot be met without reductions in immunization inequity and in particular reaching zero-dose children.
The objective of this panel is to describe a multi-country assessment that used novel approaches to identify and unmask the causes of immunization inequity, and to co-create context-appropriate solutions by engaging deeply with caregivers, community members, civil society, health workers, and other health system actors.
Presenters from the Democratic Republic of Congo, Mozambique and Nigeria will describe how they applied participatory action research, intersectionality, and human-centered design lenses, working together with community and government stakeholders, to build an understanding of the causes of inequity through the perspectives of those most affected.
Presenters will describe the findings of this process, including that caregivers of zero-dose and under-immunized children faced multiple intersecting and interacting barriers related to gender, poverty, geographic access, and service experience.
Panelists will share lessons learned from co-creating locally-relevant solutions with caregivers and communities to strengthen immunization and PHC services, including how health systems managers and technical partners can feasibly integrate HCD and intersectionality mindsets into existing planning and assessment processes to define and identify local inequities.
Presenters
- Dr. Betuel Sigauque, Country lead, MOMENTUM Routine Immunization Transformation and Equity (Mozambique)
- Salva Mulongo, Deputy Country Lead, MOMENTUM Routine Immunization Transformation and Equity (DRC)
- Yakubu Joel Cherima, Country Lead, MOMENTUM Routine Immunization Transformation and Equity (Nigeria) Responsable national, MOMENTUM Routine Immunisation Transformation and Equity (Nigeria)
Moderator
- Olivia Nava, HCD and Co-Creation Lead, MOMENTUM Routine Immunization Transformation and Equity
Authors: Wafula G1, Opiyo M1, Odhus C2,; Amihanda R1, Affiliations: Kisumu County Department of Health (1), UNICEF (2)
Background: Childhood is a crucial stage of development and lays the foundation for future health, wellbeing and success in life. Nurturing care, refers to the provision of responsive caregiving, support and protection to children, is essential in ensuring optimal childhood outcomes. However, many children living in rural communities in developing countries, including Kenya, face significant health challenges that undermine their ability to reach their full potential. Nurturing care if well practiced is an important way towards achieving UHC.
Purpose: Explore effectiveness of Nurturing Care interventions delivered by CHWs in improving child health outcomes in rural Kenya. It aims to demonstrate effective strategies for promoting child health and development in rural settings.
Problem statement: In Sub-Saharan Africa and in Kenya, the wider rural communities have been disadvantaged in accessing quality health care due to their location. Research shows that children born in these communities often have developmental challenges and therefore not achieving their full potential in life.
Interventions: Nurturing care training was done between year 2021 and 2022. 260 Community Health Workers were trained for 3 days. Methodology Surveys done between October 2022 and January 2023.
Qualitative Method: -Focused group discussions were done in Households to ascertain the impact and effectiveness of nurturing care. Quantitative method: - Survey was conducted in East Seme ward, Seme sub county with a total of 7389 Households. 800 households were randomly sampled and questionnaires administered. Data extracted from KHIS.
Results:
1. 70% of households visited had homemade children play items.
2. 86% of respondents had satisfactory knowledge on nurturing care.
3. Media documentary shows effectiveness of CHWS in implementation of nurturing care in households visited as per the FGDs.
4. Data from the Kenya health information system shows an increase in household visitations by CHWS: 2020- 48,215,2021-276,551 and 2022-299,362.
Conclusion: More investments should be directed towards supporting CHWS and caregivers so as to enable children reach their full potential.
Presenters
- Mrs. Maurine Opiyo, CHWS supervisor, County Department of Health, County Government of Kisumu, Kenya
- Bella Amihanda
Moderator
- Mr. Gilbert Wafula, CHWS Supervisor
Aim: In this session we will share innovative examples of improved counseling approaches tested in Zambia, the Democratic Republic of the Congo, and Nigeria that improve facility-based health workers’ and community health workers skills in counseling that is focused on deeply engaging with caregivers.
Objective: Exchange promising social and behavior change programmatic approaches to reach children and improve nutritional outcomes.
Background: Quality counseling from trained providers is critical to inform and motivate caregivers to take a wide range of actions: feeding children according to nutrition guidelines, administering prescribed medications, and seeking follow-up care when appropriate (among others). Training and job aids often steer providers toward detailed, sophisticated messages that may be appropriate for unhurried conversations, but don’t match the time constraints of many health facilities. And when providers doubt a caregiver’s ability or willingness to follow through, they can be discouraged from counseling at all. For caregivers, receiving a large amount of information at once can be overwhelming and hard to act on, particularly for those who are less educated, feel intimidated, or face practical and financial challenges to action. This perpetuates inequities by failing to support caregivers to take the actions that will nurture their children’s health and growth. We will highlight examples of “bite sized” counseling in the DRC and Zambia from the Breakthrough ACTION and USAID Advancing Nutrition projects, along with guidance on how they might be adapted to other contexts. 1) A simple message on both benefits of exclusive breastfeeding and risks of food and water to infants, along with a sticker reminding providers to say it in routine visits. 2) A “food prescription” elevating the importance of feeding alongside medicine to help a young child recover from illness, along with the motivating message that every bite counts. 3) An emergency planning prompt with simple cues for when to seek care for sick children and guidance for caregivers to develop a concrete plan for how they will seek care. Examples will be shared alongside the formative research and behavioral science insights on which they were based, which guided how messages were pared down to match what providers and caregivers found realistic and motivational while remaining clinically accurate.
Approach: Desk review and digital ethnography provided insights into nutrition counselling challenges. Qualitative interviews validated findings. Research informed the design of a novel CHW nutrition tool.
Solution: Tailored counselling tools were developed to educate, empower, and activate caregivers for improved complementary feeding. Empathways, Assessing Caregiver's Knowledge, Counselling flow, Action planner, Card games, and trivia engage caregivers to promote practical learning.
Impact: Collaboration with CHWs and communities offers promising solutions to improve nutrition counselling. Efforts aim to enhance feeding practices and child well-being.
Learnings: Gamification facilitated open conversations, but CHWs hesitated to share personal stories. Compassionate counselling requires a distinct skill set.
USAID-funded Breakthrough ACTION in collaboration with USAID Advancing Nutrition
Presenters
- Emily Zimmerman, Managing Director, ideas42
- Shittu Abdu- Aguye, Senior Deputy Project Director-Integrated Social Behavior Change; Breakthrough ACTION- Nigeria
- Angela Samba, Senior Maternal, Newborn and Child Health + Nutrition Advisor
Moderator
- Lynn Van Lith, Technical Director—Breakthrough ACTION, Johns Hopkins Center for Communication Programs
Addressing inequities in child health requires a parallel focus on service delivery and access to key commodities. Pneumonia accounts for 14% of all deaths of children under five with the highest burden falling disproportionately on low and middle income countries (LMICs)1,2.
However, pneumonia has historically not received the same level of donor support as other disease areas, receiving only 7% of total donor support given to malaria and HIV/AIDS between 2007 and 20183. While the existence of amox DT, a cost-effective, WHO-recommended antibiotic is available, access to this life-saving commodity remains abysmally low in many LMICs1.
In Ethiopia and Tanzania, comprehensive technical assistance (TA) supported the governments to strategically address child health financing inequities through: (i) mobilization of donor funding to avert financing cliffs; (ii) development of co-financing agreements to catalyze domestic financing, and (iii) gradual mobilization of domestic resources to promote sustainable financing.
Between 2016 and 2023, Ethiopia and Tanzania have gradually increased their domestic mobilization resources for Amox DT from $0 to $1.3M and $0.4M respectively. The continued development of domestic resource utilization and mobilization strategies as well as other sustainable financing options such as integration into national health insurance schemes and private sector scale-up has resulted in amox DT now being fully funded through domestically mobilized resources in both countries.
Combined with additional TA to address regulatory, supply, and demand side barriers, this has resulted in improved availability and reduced stockouts of amox DT across public health facilities. Availability increased from 56% in 2015 to 93% in 2019 in Ethiopia and from 25% in 2016 to 90% in 2022 in Tanzania and stockouts reduced by ~75% in both countries.
Presenters
- Dr. Felix Bandala, Assistant Director for Newborn, Child and Adolescent Health, Ministry of Health Tanzania
- Meles Solomon, National Newborn & Child Health Desk Head, Ministry of Health Ethiopia
- Samantha Durdock, Senior Program Officer, Results for Development
- Yewedalem Tesfaye, Associate Director, Results for Development
Moderator
- Nelsha Haji, Senior Program Officer, Results for Development
We propose a moderated discussion to share Uganda’s experiences scaling up IMNCI, considerations to achieve critical numbers of trained health workers, strategies to foster inter-agency cooperation, and approaches to integrate quality improvement practices (QI) to sustain training gains.
Background: Uganda’s under-five child mortality rate remains high at 42 deaths per 1,000 live births with persistent subnational disparities. Scaling coverage of high-impact interventions for common childhood illnesses is a priority for the Ministry of Health (MoH).
In 1996, Uganda adapted the 11-day Integrated Management of Childhood Illness training, which was later expanded to include newborns, WHO updates, and renamed Integrated Management of Newborn and Childhood Illnesses (IMNCI).
The lengthy, classroom-based training was resource-intensive and kept critical cadres from service delivery. By 2017, reach was limited to around 83 HWs in four districts.
Implementation Approach: In 2017, MoH, WHO, UNICEF, and USAID modified and tested the training delivery to a “short, interrupted course” (SIC), which involved a 2½-day face-to-face orientation, 2-weeks of self-study and case practices, and 1½-day of review and synthesis. The SIC reduced the cost of training and service disruption and increased HWs trained per facility. Further, QI practices focused on establishing Oral Rehydration Therapy corners, tracking appropriate pneumonia treatment, malaria test-and-treat, and integrating ORS+zinc co-packs for diarrhea management were incorporated to help sustain training gains by supporting HWs to assess and address identified gaps continuously. Using this approach with stakeholder collaboration, IMNCI was scaled to 26 additional districts and 1,024 HWs between 2019 to 2022.
Lessons learned/Conclusion: Modifying the training delivery to achieve critical numbers of trained HWs combined with integrated QI practices enabled the scale-up of IMNCI in Uganda. This work remains a priority, and MoH, USAID, and UNICEF will target implementation in districts with the highest burden of child mortality.
Presenters
- Mrs. Agnes Namagembe, Maternal Child Health Specialist, FHI 360/ USAID Maternal Child Health and Nutrition Activity Uganda
- Dr. Peter Waiswa, Professor, Makerere University, School of Public Health
- Dr. Bodo Bongomin, National Professional Officer - Child and Adolescent Health, World Health Organization Uganda
- Dr. Jesca Nsungwa, Commissioner of Reproductive and Child Health, Ministry of Health
- Dr. Emmanuel Mugisa, Program Management Specialist for Child Health and Nutrition, USAID, Uganda
The key to successful grant writing is the ability to communicate vision and capacity for project implementation. These skills are critical for obtaining funding and/or in-kind support to establish and sustain impactful projects and programs. This workshop aims to prepare proposal and grant writers with the knowledge and skills to approach different kinds of grant writing opportunities. Faculty from the American Academy of Pediatrics Global Health Office and International Community Access to Child Health (ICATCH) Program will share their expertise in research, programmatic and community-focused grants.
The learning objectives are:
1. Understand different types of grant programs and audience for proposals
2. Identify the components of a well-organized grant proposal
3. Practice drafting a problem statement and other aspects of a potential proposal
First participants will receive a brief overview on grant writing that will include how to: (1) Identify grant opportunities; (2) Research the granting organization; (3) Review the proposal requirements; (4) Write an aims statement; (5) Include community partners in the proposal development process; (6) Align project activities with budget requests; and (7) Measure and evaluate planned activities.
Then participants will interact in small group breakouts led by faculty with expertise in research, foundation and community grants on workshopping generic proposal ideas. This will be followed by a large group discussion to identify and summarize key points. Participants will leave with a compiled list of grant writing resources.
Presenters
- Dr. Rachel Umoren Program Director, ICATCH Program
- Dr. Ann Behrmann, Immediate Past Program Director, ICATCH Program
- Dr. Leslie Cordes, General Pediatrician, Lurie Children's Hospital, Chicago
The purpose of this session is to build the capacity of planners and managers to calculate the cost of community child health services within the context of community health care programs and to develop investment cases that can be used for advocacy and planning.
Participants will be provided with an overview of the process of costing using the Community Health Planning and Costing Tool. They will learn about type of data required, how data are entered into the tool, what kinds of reports are produced, and how what-if-analysis can be carried out. They will also learn how to use the results to develop an investment case. The session will involve the presentation of an overview of the process of carrying out the costing and preparing an investment case as well as a walk-through of key elements of the tool.
Links to tool webpages:
https://msh.org/resources/community-health-planning-and-costing-tool-version-20-handbook/
https://msh.org/projects/community-health-planning-and-costing/
To request access please email: fintools@msh.org
Presenters
- Professor David Collins, Independent Consultant, Boston University School of Public Health
- Colin Gilmartin, Principal Technical Advisor, Health Economics and Financing, Management Sciences for Health
Objectives: After attending the session, attendees will be able to:
1. Understand the relevance of Proprietary Patent Medical Vendors and Community Pharmacists in child health care for underserved communities of Northern Nigeria.
2. Understand how Community Health Information Systems (CHMIS) is rolled out in Nigeria and reporting of key child health indicators.
3. Understand PPMVs and CPs can provide quality childcare services through capacity building, mentoring and supervision.
This session will explore how a community health information system can be used to improve accountability of child health services among Patent and Proprietary Medicine Vendors and Community Pharmacists; a critical frontline healthcare cadre for many low-resource and remote households throughout Nigeria.
The session will discuss how PPMVs, and CPs can be fully effective to provide quality childcare services.
The session will also explore ways to ensure the data is used to monitor and improve the quality and availability of services for children.
The session will share experiences/lessons learned and discuss recommendations for implementing a community health information system for PPMVs and CPs
Topics: Capacity building, onsite mentoring, monitoring, and reporting of services, quality of care and ways to ensure data accuracy, accountability of frontline services that serve the poor and provide equitable care.
Presenters
- Dr. Mohammed Zainab, Integrated Primary Health Care Advisor - USAID IHP Nigeria
- Tosin Akingbemisilu, Senior ICT Specialist - USAID IHP Nigeria
- Chinwoke Isiguzo, Director, Monitoring, Evaluation and Learning - Palladium
Moderator
- Angie Stene, Director, Palladium
During the last decades the world has experienced a progressive decrease in newborn and child mortality. According to the latest UN-IGME report, the global under-5 mortality rate (U5MR) halved during the 2000-2021 period, going from 76 to 38 deaths per 1,000 livebirths (L.B.) The global newborn mortality rate (NMR) has followed a similar trend, going from 31 to 18 deaths per 1,000 L.B.
Despite this improvement, the reduction in mortality is uneven between and within countries, where most of the burden is concentrated in low- and middle-incomes countries (LMICs), particularly in Sub-Saharan Africa and South Asia, as well as in rural and distant communities, the poor, and importantly, in humanitarian settings. For example, out of the 5 million global deaths of children under 5 in 2021, 55% (2.7 million) took place in humanitarian settings. Similarly, out of the 2.3 million neonatal deaths, 1.6 million, or nearly 50%, took place in a country facing a humanitarian crisis, as per OCHA’s classification. Thus, SDG 3.2 will not be achieved unless efforts are focused to expand access and improve health services for children living in emergency contexts.
Providing health services in emergency and humanitarian contexts, however, presents several challenges due to the destruction of infrastructure, disruption of health, other social services, and supply chains, limited healthcare staff capacity, hazards for healthcare providers and patients, and frequent movement of populations.
The proposed presentation will explore key child health indicators in humanitarian and fragile settings, including mortality trends as well as some other metrics included in the Health SDGs, to better understand humanitarian-related inequities in health and serve as an advocacy tool to prioritize child health and social programming in these contexts.
Presenters
- Ralf Moreno, Health Specialist, Health in Emergencies and Humanitarian Settings unit, UNICEF H.Q.
- James McQuen Patterson, Chief for Health in Emergencies and Humanitarian Settings, UNICEF
The child survival action (CSA) initiative calls national, regional, and global partners to end preventable child deaths and accelerate action in the 54 countries not on track to meet the 2030 Sustainable Development Goals’ under-five mortality target. Within these 54 countries, deaths in the 1-59 month period of life are a substantial portion of all under-five deaths.
The CSA initiative is developing a results framework to stimulate action and allow countries to track their progress. To ensure alignment and harmonization, the group mapped child survival indicators tracked in existing initiatives and recommended in global guidance. Impact indicators in the results framework include under-five mortality, mortality in the 1-59 month period, and prevalence of wasting and stunting.
Outcomes selected for the framework include coverage of key preventative interventions, such as nutrition practices, immunization, and use of insecticide treated nets, and coverage of illness management practices, such as zinc and ORS for diarrhea, use of malaria diagnostics for fever and careseeking for fever and symptoms of acute respiratory illness.
Equity and quality of child health care are included as key outcome measures. The initiative recommends examining impact and coverage indicators amongst the poorest children within a country. Fewer global validated measures and data reporting platforms exist for tracking quality of care; the CSA recommends using the WHO pediatric quality of care indicators accompanied by a robust learning agenda for measurement improvement.
Implementation milestones and programmatic indicators are being developed and vetted for 1) governance, national plans, and financing; 2) data and accountability; 3) service delivery systems; 4) community and family engagement; and 5) partnerships. The final CSA framework and associated analytics can be used by global, regional, and country stakeholders to focus attention on the unfinished child survival agenda, mobilize resources, and plan and adjust strategies and implementation approaches.
Presenters
- Lara Vaz, MOMENTUM Knowledge Accelerator, Population Reference Bureau
- Dr. Kate Gilroy, MOMENTUM Knowledge Accelerator, John Snow, Inc
- Dr. Dyness Kasungami, Project Director, Child Health Task Force
- Jennifer Harris Requejo, Global Financing Facility (GFF), World Bank Group and Johns Hopkins Bloomberg School of Public Health
- Dr. Shane Khan, Consultant, Child Survival Action Metrics Working Group
After sharing approaches and tools to identifying, addressing, and measuring equity and attending skills-building sessions, participants will be inspired to go back and program differently. This Plenary will offer reflections; recognize the shared solutions and innovations; and highlight emerging issues, gaps, and barriers to progress. It will also challenge child health partners to employ the Task Force platform as a mechanism to share homegrown transformational stories that became possible because of the re-commitment to ending preventable child deaths.
Presenters
- Dr. Queen Dube PhD, Chief of Health Services, Ministry of Health Malawi
- Dr. Dyness Kasungami, Project Director, Child Health Task Force
- Dr. Sangita Yadav, Professor, HIMSR and HAHC, Maulana Azad Medical College, New Delhi
- Dr. Lu Wei Pearson, Associate Director for Maternal and Newborn Child Health, UNICEF
Moderator
- Mercy Juma, BBC News East Africa Correspondent